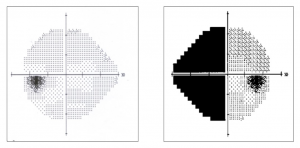
A 57 year old asymptomatic woman was referred for a glaucoma evaluation due to elevated intraocular pressure (IOP). Her visual acuity was 20/20 in each eye and pupils were normal without afferent defect. Her IOP was 25 mm Hg OD and 24 mm Hg OS. Her optic nerves were symmetrically cupped at 0.6/0.6 OD and 0.7/0.7 OS with no evidence of rim thinning, pallor, focal rim defects, hemorrhage, or retinal nerve fiber layer (RNFL) defects. Additionally she passed color vision screening in each eye. Optic coherence tomography revealed a robust and normal RNFL and ganglion cell analysis in each eye. However, threshold perimetry presented unexpected results: Her left visual field was perfectly normal, but her right had a complete left nasal hemianopic defect exquisitely respecting the vertical midline.
Such findings should prompt an investigation for a neurologic, non-glaucomatous etiology. Confounding was the fact that the field defect was only present in her right eye with normal results in her left. Chiasmal and retrochiasmal causes virtually always have bilateral visual field defects respecting the vertical midline which assist with lesion localization. Unilateral visual field loss localizes to an etiology anterior to the chiasm. However, every aspect of her anterior visual pathway including acuity, pupils, color perception, RNFL and optic disc were all normal. So, where is the problem occurring?
Chiasmal and retrochiasmal lesions are expected to have bilateral visual field loss. If the lesion occurs at the chiasm, the defect will be bitemporal. Lesions posterior to the chiasm will present with hemianopic defects occurring on the side opposite the lesion. The more posterior the lesion, the more congruous the visual field defect. A left superior quadrantanopsia would indicate a right temporal lobe lesion and a left inferior quadrantanopsia localizes to the right parietal lobe. Visual field loss occurring in one eye only indicates an issue anterior to the chiasm. However, such issues rarely, if ever, respect the vertical midline as seen here. Additionally, such lesions will also present with some readily identifiable abnormality in visual acuity, color perception, afferent pupillary response, optic disc health, or RNFL structure. This woman had no such findings.
When faced with a situation that shouldn’t exist, alternate explanations should be sought. In this case, no advanced neuroimaging was needed to ascertain the cause. After a brief discussion, it was determined that the perimetrist who administered the test did not choose the proper words when instructing the patient (who had never previously taken a visual field test). Instead of telling the patient that she was going to test the right eye first, the perimetrist instead said that she was going to test the right side first. Thus, the patient was under the impression that she should ignore all stimuli presented in her left visual field, which she did exquisitely well. Fortunately, the patient didn’t do the same thing when testing the left eye, otherwise she would have likely undergone a lot of unnecessary testing. Repeat perimetry with proper instruction resulted in a perfectly normal visual field in each eye as well as a few laughs.
Always remember that a patient can fake vision loss, but they can’t fake a pupil defect or RNFL abnormality.